腎上腺切除後腎上腺機能不全
朱信誠、高偉棠
台北醫學大學-部立雙和醫院泌尿科
Case report- Acute Adrenal Insufficiency After Unilateral Adrenalectomy in Metastatic Lung adenocarcinoma
Chu-Hsin Cheng, Wei-Tang Kao
Department of Urology, Taipei Medical University-Shuang Ho Hospital, Taipei, Taiwan
Backgroud:
Adrenal crisis, also termed acute adrenal insufficiency is an acute life-threatening condition, which is precipitated by an internal or external process in the setting of known or unknown lack of production of the adrenal hormone, glucocorticoid. Early identification and prompt management can save the patient's life and impact survival. The clinicians should be able to identified adrenal insufficiency and adrenal crisis since the adrenal crisis is fatal if left untreated.
The predominant manifestation of adrenal crisis is shock, but the patients often have nonspecific symptoms such as anorexia, nausea, vomiting, abdominal pain, weakness, fatigue, lethargy, fever, confusion, or coma. Hence, we present a case of acute adrenal insufficiency after unilateral adrenalectomy.
Case Report:
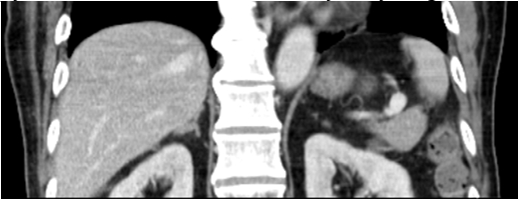
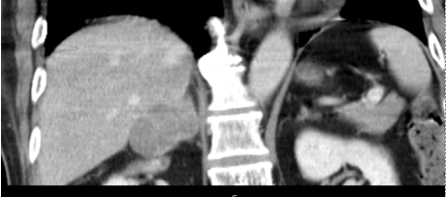
A 67 years old male presented with an enlarging right adrenal mass over 17 months. The maximal diameter of the mass was growing form 1.4cm (Figure 1) to 4.7cm (Figure 4). Past history including 1.Lung adenocarcinoma (T2N1M1b), stage IV with brain and bone metastasis status post chemotherapy 2.Old left middle cerebral artery territory infarction with right hemiparesis and aphasia 3.Hypertension under medication control 4.Type 2 diabetes mellitus. Symptoms such as hypertension, dizziness, palpitation, were denied. No signs of buffalo hump, purple striae, or moon face. Electrolyte levels such as sodium, and potassium were normal. Right side laparoscopic adrenalectomy was performed smoothly. EBL was 50ml. Drain color was light reddish. However, hypotension was noted at post-operative room. After fluid challenge with normal saline 400ml and lactate ringer 500ml, blood pressure was 100/78mmHg. The patient was then sent to ordinary ward. However, hypotension with consciousness disturbance was noted again by duty doctor. Methylprednisolone 100mg and Hydrocortisone 200mg were injected intravenously. After an hour, the symptoms improved dramatically. ATCH level was 2.0 pg/mL, which was below normal level. Acute adrenal crisis with shock was diagnosed. Hydrocortisone dose was tapered gradually, and no other symptoms noted. The patient was discharged under stable condition.
Conclusion:
In the setting of unilateral adrenal metastases, adrenal insufficiency is unlikely and typically does not need evaluation. However, in patients with a history of cancer and use of glucocorticoids as part of chemotherapy regimen or otherwise over the last year, the possibility of glucocorticoid-related adrenal suppression should be considered. In this case, the adrenal mass was thought to be metastatic form lung adenocarcinoma, which was proven by surgical histopathology. The patient received Dexamethasone 2mg chemotherapy as part of chemotherapy regimen, which was relevant to this episode. Furthermore, adrenal crisis is triggered by physiological stress, such as surgery, or trauma. In conclusion, adrenal crisis is an acute life-threatening condition, and the treatment with hydrocortisone should not be delayed by diagnostic tests.
 |
 |
|
Figure 1.
|
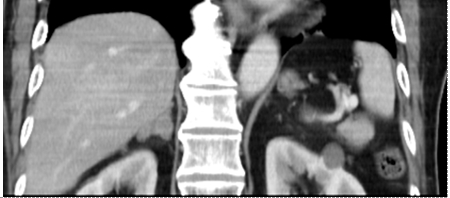
Figure 2.
|
 |
 |
|
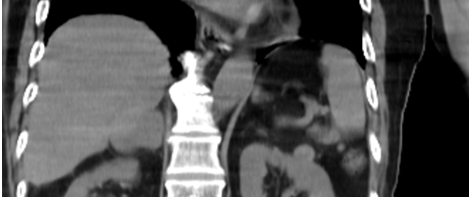
Figure 3.
|
Figure 4.
|
|
Figure 1. non-contrast CT scan in Sep 2018
Figure 2. non-contrast CT scan in Feb 2019, maximal diameter was 3.3cm
Figure 3. non-contrast CT scan in Oct 2019, maximal diameter was 4.0cm
Figure 4. non-contrast CT scan in Jan 2020, maximal diameter was 4.7cm
|
|
附件: