NPD64: Nontraumatic Page kidney– A case report and literature review
一位經過放射治療後復發的後腹腔腫瘤患者在下腔靜脈切除手術與多處腸道切除手術後的預後-案例報告
徐明蔚、楊啟瑞
中國醫藥大學附設醫院 泌尿部
Outcomes after IVC resection without reconstruction and multiple bowel resections in a patient with recurrent retroperitoneal sarcoma after radiation therapy
Ming-Wei Hsu, Chi-Rei Yang
Department of Urology, China Medical University Hospital, Taichung, Taiwan
While complete gross resection is considered the only curative option for recurrent retroperitoneal sarcoma, the chance of achieving long-term disease-free survival is limited, and this must be taken into account during a multidisciplinary evaluation. The involvement of the IVC in retroperitoneal malignancies is a rare occurrence, and the prognosis is generally poor. R0 resection with vascular resection, if necessary, is the only potentially curative treatment. However, there is no consensus on whether to perform IVC resection with or without venous reconstruction. In addition, chronic radiation injury to the intestine can lead to capillary fibrosis, and the decision to resect or bypass the affected bowel segment depends on the relative risks of anastomotic leak and mortality. We will present a case of recurrent MPNST after radiation therapy, in which the patient was successfully discharged following IVC resection without reconstruction and multiple bowel resections.
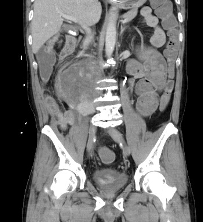
A 56-year-old man had a history of right retroperitoneal malignant peripheral nerve sheath tumor. He initially presented with abdominal pain three years ago and a right retroperitoneal tumor was diagnosed. He underwent laparoscopic resection, and subsequent pathology revealed MPNST, pT4N0, cM0. He received adjuvant chemotherapy with Gemcitabine + Docetaxel for three doses. However, local recurrence emerged over the paracolic gutter, and right retroperitoneum on 2020-8/24. As a result, he underwent palliative radiotherapy (5040cGy/28Fr), followed by Pazopanib and then AIM x 6 (June 4, 2021 to September 21, 2021). Another tumor resection was performed, but progressive disease was still observed in 2022. The patient was then referred to CMUH, where a CT scan of the abdomen revealed one 108 mm recurrent tumor in the right retroperitoneum with involvement of the spine, IVC, right psoas muscle, and right ureter, which caused right hydronephrosis.(Figure 1) Additionally, another 60 mm metastatic lesion was found in the right lower abdomen, with adjacent small bowel involvement, leading to small bowel obstruction. Inferior vena cavagram showed multiple collateral veins from bilateral iliac vessels.
During the surgery, retroperitoneal tumors had invaded the right ureter, spine, psoas muscle, IVC, colon and small bowels.We performed retroperitoneal tumor resection (figure 2) including right nephrectomy, adrenectomy, IVC resection(supra-renal and infrarenal), right colectomy with ileocolostomy, primary closure of sigmoid colon perforation, duodenum partial resection with tumor with GJ bypass, anterior partial disectomy L2/3/4/5 and anterior partial corpectomy L2/3/4/5. Initially, the patient experienced bilateral lower limb edema, but it resolved after one month without the need for anticoagulation. Furthermore, three intestinal anastomosis leaks were identified after the operation, and drainage tubes were inserted and kept regular revision. After three months of drainage, the anastomosis site had healed, and the patient was able to resume normal intake.
 .
. 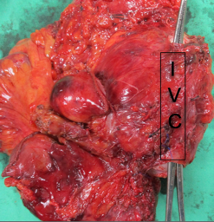
Figure 1 and figure 2
Conclusion
It is considered an acceptable option to perform IVC resection without reconstruction in patients with retroperitoneal tumors that have invaded the IVC, provided that collateral circulations have been established. For patients who have undergone radiation therapy, there is a higher risk of anastomosis leak associated with intestinal surgery. However, with prolonged drainage, wound healing can eventually occur.