以局部侵襲性表現之黄色肉芽肿性肾盂肾炎:案例報告
黃欣媚,姜秉均,黃旭澤
財團法人新店耕莘醫院
Xanthogranulomatous pyelonephritis presenting as “locally advanced” renalneoplasm : Case report.
Wong Shin Mei, Bing-Juin Chiang, Hsu-Che Huang.
Division of Urology, Department of surgery, Cardinal Tien hospital, Taipei, Taiwan.
Introduction
Originally described by Schlagenhaufer in 1916, xanthogranulomatous pyelonephritis is a rare chronic kidney infection associated with severe renal destruction. It is more common in woman than man at the age 40-60. Most patients presented with chronically ill, flank pain, bacteriuria, fever and it usually associated to renal stone and UTI. Common pathogens associated to XGP are Proteus and E.coli. CT scan is the most suitable radiographic technique in evaluating XGP. In particular, demonstrating the extent of adjacent organ involvement. MRI usually used in patient with poor renal function, but MRI did not provide better diagnostic benefits in XGP.
Case presentation
A 59-year-old female, with history of diabetes mellitus, hypertension, chronic obstructive pulmonary disease under regular oral corticosteroids and obesity(BMI 38) presented with low grade fever, right flank pain and general malaise for few days. She first consulted in August 2019 and physical examination revealed right flank knocking pain. CT scan disclosed a 3-cm hemorrhagic cyst. 1-week antibiotic was prescribed, the patient had improvement of her symptoms. However, the patient presented again at our outpatient clinic three months later with relapsed of right flank pain and progressive general weakness. Follow up CT scan revealed a large renal mass. There was extension beyond renal capsule and extending to the liver and psoas muscle. Imaging findings were consisted with a clinical diagnosis of invasive renal cell carcinoma. The patient underwent a right radical nephrectomy with partial hepatectomy and extended tumor excision. Pathology revealed xanthogranulomatous inflammation in all specimens, no malignancy was found. Receiving prolong antimicrobial therapy, the patient discharged smoothly two weeks after surgery.

CT scan with and without contrast, showing right renal hemorrhagic cyst. (Aug 2019)
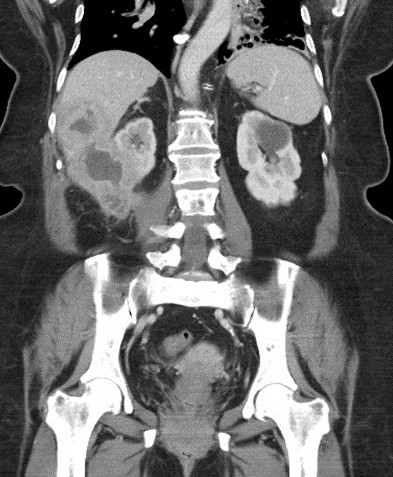 |
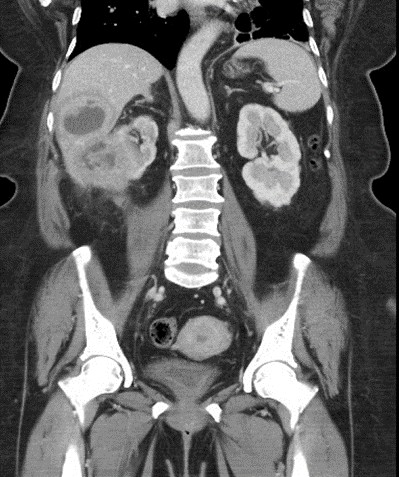
CT scan: 3-month later, showing right renal mass, mimicking renal cell carcinoma with liver and psoias invasion.(Nov 2019)
Discussion
We present a rare case of xanthogranulomatous pyelonephritis with extension to surrounding viscera, originally diagnosed as an RCC. This is rare but importance case of a large renal inflammatory lesion mimicking locally advanced tumor and progressive rapidly in a short period of time. XGP has been named as a great mimicker owing to more often misdiagnosed clinically and radiographically as renal malignancy. To the best of our knowledge, XGP is typically related to infection, obstructive uropathy and nephrolithiasis-. Most common pathogen related to infection has been reported as E.coli, Proteus, etc. Up to 80% of patient with presence of renal calculi.
However, in this case, the patient presented with rapid progression renal tumor and large portion of liver involvement in only 3 months of time. The patient felt general weakness, flank soreness and barely fever. It is noteworthy that the patient has been regularly taking corticosteroid for her respiratory condition for more than 5 years, this may mask the symptoms of infection, inflammation. Furthermore, absence of nephrolithiasis in this case lead to incorrect diagnosis. Diagnosis is challenging due to the non-specific features. Nevertheless, if malignancy could not be excluded, surgical excision should be performed. Surgical excision is the only definitive treatment, it was dangerous for this patient with local organ involvement. Nephrectomy is the criterion standard treatment for XGP as well as remove all the inflammatory tissue.
Conclusion
It is crucial to differentiate aggressive xanthogranulomatous pyelonephritis from renal cell carcinoma, which in indistinguishable clinically and radiographically. Preoperative biopsy is not sufficient to exclude malignancy. Medical treatment or less invasive procedure such as incision or drainage may not suitable for this rapid progressive case.
附件: