特別之雙套輸尿管病例分享
劉瑞文、陳冠州
衛生福利部立雙和醫院 泌尿科
Special duplication collection system case
Liu Jui Wen, Chen Guan Zhou
Department of Urology, Shuang Ho hospital, Taipei Medical University, Taipei, Taiwan
Introduction: Duplication collection system is not such rare condition for urologist. We are sharing one special case who upper duplication collection system outlet is located in front of verumontanum. This case report showed how the initial work up and further management are done.
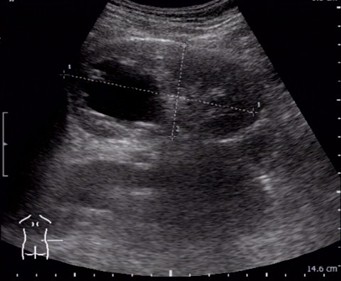
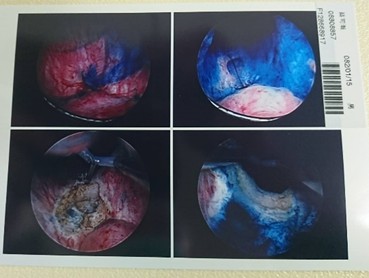
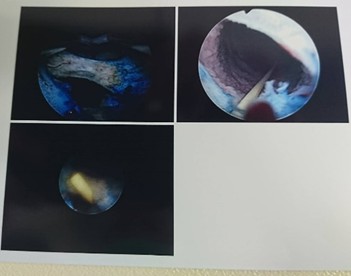
Case report: This 25 years old male patient denied chronic or systemic disease. There wasn’t family history of malignancy or hereditary disease. Renal echo showed right hydronephrosis while health examination. So he came to our out-patient department for help. Physical examination showed no obvious abnormal finding. Follow up renal echo showed hydronephrosis or renal cyst. KUB showed no obvious stone like lesion. Biochemistry showed Cr: 1.02, eGFR:94.6. Abdominal CT showed right hydroureteronephrosis at least to visible mid-ureter. Then admission for ureteroscopic examination was suggested and he accepted. Pre-operation biochemistry showed PT/INR prolonged (14.7/1.21), hypokalemia(3.3), others value within normal limit. Operation finding showed duplication of ureter of right side, only one ureteral outlet can be found. So right side percutaneous nephrostomy pigtail drainage was inserted. Post operation antegrade pyelography and CT urology showed duplex collecting system and right hydroureter with UVJ stricture. Then second operation as transurethral incision according image finding was done. Operation finding showed the lower total obstruction ureteral outlet in front of verumontanum and double J catheter was inserted. Follow up renal echo showed hydronephrosis was subsided gradually.
 |
 |
|
Pre-OP right side renal echo
|
Pre-OP KUB
|
 |
 |
|
Pre-OP abdominal CT
|
Post 1st operation antegrade pyelography
|
 |
 |
|
Post 1st operation CTU
|
Post 1st operation CTU
|
 |
 |
|
2nd operation finding
|
2nd operation finding
|
Discussion: Duplication of collection occur over 1% of population, 10% of children. Pathophysiology showed Lower pole vesicoureteral reflux, upper pole obstruction. Common clinical presentation showed hydronephrosis, urinary tract infection, hematuria, abdominal pain. Incontinence can be found in female population due to ectopic meatus. Physical examination showed palpable abdominal mass, ectopic meatus. The main finding of anatomy was Weighert-Meyer rule. A ureterocele is a cystic dilatation of the terminal intravesical ureter. Ureteroceles that are entirely contained within the bladder are considered intravesical. A ureterocele is considered ectopic if any portion is permanently situated at the bladder neck or the urethra, regardless of the position of the orifice. Work up and treatment was noted as above information.
附件: