經腎盂切口腎臟鏡取石術處理”橡皮樣”鹿角結石-個案報告及文獻回顧
楊涵中1、陳卷書1,2
1臺中榮總泌尿外科 2中山醫學大學臨床醫學研究所
Per-Pyelotomic NephroLithotomy (PPNL) for “rubbery” staghorn stones of both kidneys – Case report and literature review.
Han-ChungYang1, Chuan-Shu Chen1,2
1 Division of Urology, Department of Surgery, Taichung Veterans General Hospital, Taichung, Taiwan, 2 Institute of Medicine, Chung Shan Medical University, Taichung, Taiwan,
Abstract:
Management of renal staghorn stones is always challenging. Standard treatments for renal staghorn stones include percutaneous nephrolithotomy(PCNL), retrograde intrarenal surgery(RIRS), laparoscopy and open surgery. We present a case of 55-year-old male with bilateral renal staghorn stones which cannot be successfully managed with PCNL and RIRS due to a large stone burden and rubbery texture of the stone. Alternatively, PPNL including open pyelotomy combined with nephroscope results in nearly complete stone removal on both sides.
Case presentation:
This 55-year-old male was diagnosed with bilateral renal staghorn stones three years ago. He underwent several unsuccessful surgeries in the past three years including PCNL and RIRS before presenting to our ED with fever, bilateral flank pain and turbid urine. Laboratory data showed leukocytosis, impaired kidney function (sCr:4.77mg/dL). Computed tomography scan revealed bilateral complete staghorn stones and left ureteral stone with hydroneprhosis. The patient was admitted for infection control and pre-operative preparations.
During operation, the patient was placed on semi-flank position with elevation of left side. A 10 cm transverse incision over left upper quadrant of abdomen was made at the level of 11th rib. The abdominal wall muscle and the peritoneum was identified and dissected with caution to maintain a retro-peritoneum route. The lower pole of left kidney, ureter and renal pelvis were identified. A longitudinal incision (1.5cm) was made over renal pelvis. Ureteral stone was removed first under flexible cystoscopy. An amplatz sheath was inserted into renal plevis via previous pyelotomy. Under nephroscopy and hand-assisted manipulation of kidney, stones were removed with forceps and basket piece by piece. Energy devices (such as laser and lithoclast) were less helpful because of rubbery texture of the stones. The pyelotomy was closed with 3-0 V-lock after placing double J catheter. Wound was closed layer by layer after drainage tube placed near renal hilum. The operation took approximately three hours.
The patient tolerated the operation very well with minimum blood loss. There’s no sign of urine leakage, wound infection, sepsis or deterioration of kidney function after operation. The patient was discharged on post-operative day six. After a three-week interval, the patient was re-admitted for right renal staghorn stone which was managed with identical operative technique as left side. Further CT scan showed nearly complete stone removal on both sides.
Discussion:
To date, PCNL is considered a gold standard treatment for renal staghorn stone despite the possibility for repeat procedures or post-PCNL ESWL. Once PCNL failed, repeated procedures or alternative techniques such as RIRS, pyelolithotomy, anatrophic nephrolithotomy should be considered. Our patient is not considered candidate for repeat PCNL or RIRS because of previous unsuccessful attempts. Repeated PCN insertion with tract dilatation is associated with increased risk of organ injury, bleeding, sepsis and post-operative renal dysfunction. Anatrophic nephrolithotomy may itself negatively compromise the functional condition of the surgically treated kidney. Scar formation and temporary occlusion of renal pedicles could further jeopardize the remaining renal function of our patient.
In literature review, Beata Jurkiewicz and colleagues performed similar operations on pediatric patients whose kidney stones failed initial minimally invasive procedure. Eighteen kidneys from fifteen pediatric patients underwent combined operation of pyelolithotomy with endoscopic removal of staghorn stones. Fifteen out of eighteen kidneys are stone-free at one operation and the remaining three being candidate for ESWL. No serious complication was reported in their review.
In our case, PPNL offers the advantages of preventing complications of repeated PCNL, minimizing renal parenchyma damage, increased stone free rate in case of refractory stone. PPNL was also time-saving, because these rubbery stones can only be successfully removed with forceps (mechanical force) but refractory to energy devices.
Conclusions:
PCNL is the gold-standard treatment for renal staghorn stone. Stone free rate was high and incidences of complications are acceptable. However, in complicated and refractory cases, PPNL is safe and feasible, potentially as an alternative for traditional methods.
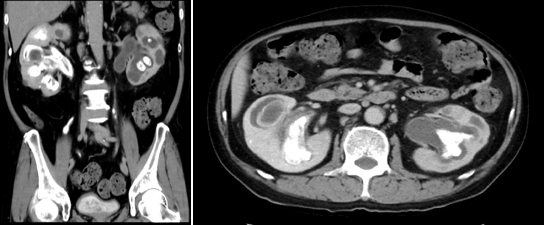
Fig1. Pre-operative CT with staghorns stones filling both calyxs.
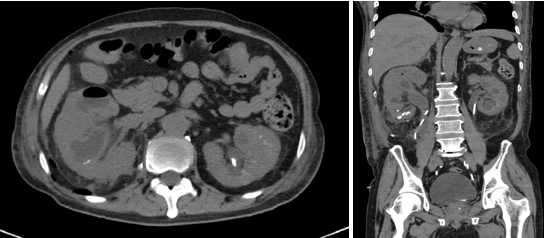
Fig2. Post-operative CT showed nearly complete stone removal.
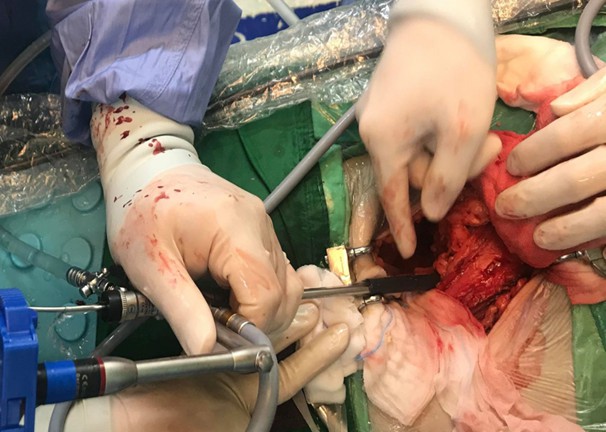
Fig.3 An amplatz sheath in renal pelvis, stone was removed under nephroscope with forceps.

Fig.4 Stone fragments.
附件: