Podium 01
個案報告:偽裝為膀胱腫瘤的息肉性膀胱炎
陳柏翰1、曾仁澍1
1台灣基督長老教會馬偕醫療財團法人馬偕紀念醫院 泌尿科
A case report: Polypoid Cystitis Masquerading Bladder Tumor
Bo-Han Chen1, Jen-Shu Tseng1
Department of Urology, MacKay Memorial Hospital, Taipei, Taiwan1
Background
Polypoid cystitis is an inflammatory reaction of bladder and usually related to irritant condition, including indwelling urethral catheter, bladder calculi, urinary outflow obstruction and colovesical fistulae. However, patient without history of these condition infrequently suffered from polypoid cystitis. Here, we shared a rare case of polypoid cystitis and our treatment course.
Case presentation
A 64-year-old woman presented with painless gross hematuria for 1 month and urinary frequency for 2 months. She had medical history of hypertension and type 2 diabetes mellitus. No dysuria or abdominal discomfort was complained. Physical examination was unremarkable, and laboratory data were normal. Urine analysis revealed 1 red blood cell and 20 white blood cells per high power field. Urine culture was negative. Renal echography revealed a huge bladder lesion without bilateral hydronephrosis. She underwent cystoscope and was found having bladder tumor over right lateral wall while bilateral ureter orifices were identified. (Figure 1) Enhanced computed tomography demonstrated an enhanced mass lesion compatible to the finding of cystoscope without perivesical invasion or lymphadenopathy was noted. (Figure 2) A complete endoscopic resection with Thulium laser was performed under the impression of bladder neoplasm. Microscopically, the resections showed fragments of urinary bladder tissue with focal reactive hyperplasia but preserved polarity and absent of marked cytological atypia or mitotic activity. Focal intraepithelial neutrophils infiltration was noted. The underlying stroma showed marked edematous and fibrotic change, with subepithelial lympoplasmacytic infiltration and occasional germinal centers formation. Areas of interstitial hemorrhage were observed. There was no evidence of carcinoma. Soft tissue tumors were unlikely due to negative result of calretinin, WT1, CD31, D2-40, S100, melan-A and HMB-45. The CD 68 stain highlights scattered histocytes. The overall picture favors inflammatory process, most likely polypoid cystitis.
After the operation, the patient’s symptoms improved. Since there is no malignancy potential, no further adjuvant therapy was prescribed.
Discussion and conclusion
Polypoid cystitis usually presents as exophytic lesion on bladder wall. Because of this characteristic, it’s difficult to distinguish polypoid cystitis and bladder malignancy under cystoscopy by visual inspection. Image study can help to survey lymphadenopathy but possess limited evidence to diagnosis. Definite diagnosis is also made only by microscopic pathological study of the resected tissue. Patient with polypoid cystitis may have hematuria or lower urinary tract syndrome. After the endoscopic resection, patients’ symptoms may subside mostly.
In conclusion, polypoid cystitis is a benign mass lesion and could suitably treated by surgical resection since its nature is difficult to determine grossly.
|
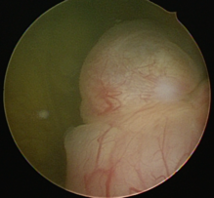
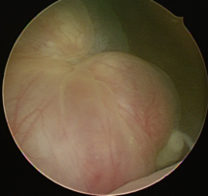
Figure 1 Cystoscope showed protruding tumor at right lateral wall. |
|
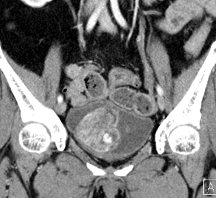
Figure 2 CT image showed an enhanced mass lesion in bladder. |