Podium 01
利用非侵入性診斷工具預測伴隨下泌尿道症狀男性膀胱出口功能障礙之亞型
張天霖、郭漢崇
佛教慈濟醫療財團法人花蓮慈濟醫院 泌尿部
Predicting the Subtypes of Bladder Outlet Dysfunction in Men with Lower Urinary Tract Symptoms Using Noninvasive Diagnostic Tools
Tien-Lin Chang, Hann-Chorng Kuo
Department of Urology, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation and Tzu Chi University, Hualien, Taiwan
Purpose: The current study aimed to develop predictive models based on noninvasive clinical parameters to facilitate the early identification and stratification of patients with suspected bladder outlet dysfunction (BOD), thereby reducing the need for invasive diagnostic procedures.
Materials and Methods: This retrospective study included 307 male patients with lower urinary tract symptoms (LUTS) refractory to medical therapy who were enrolled between January 2001 and May 2022. To assess the predictive performance of the model in an independent cohort, the dataset was randomly divided into the training set (70%) for model development and the test set (30%) for external validation. A two-stage modeling approach was adopted: Stage 1 involved detecting BOD, and stage 2 focused on identifying specific BOD subtypes. Backward stepwise logistic regression was conducted for model derivation, with internal validation performed using 5-fold cross-validation repeated 20 times. Clinical nomograms and a clinical decision-making framework were constructed based on the final modeling results.
Results: In stage 1, the derived BOD model for detecting suspected BOD incorporated maximum flow rate, voided volume, intravesical prostatic protrusion (IPP), and prostatic urethral angle as predictors. In stage 2, the derived benign prostatic obstruction (BPO) model included post‑void residual, total prostate volume, and IPP as predictors (Table 1). Both internal and external validations had good discriminative ability for the derived BOD and BPO models. However, the BOD model (0.47) had a relatively low specificity, and the BPO model (0.58) had a lower sensitivity. Thus, these findings should be considered when applying the models in clinical practice (Figure 1).
Conclusions: This stepwise strategy, which applies the high-sensitivity BOD model for initial screening, followed by the high-specificity BPO model for subtype confirmation, effectively reduced the need for videourodynamic study by limiting it to patients with non-BPO phenotypes requiring further evaluation. The results of this study revealed that using the clinical non-invasive parameters to create models can only yield a low sensitivity and low specificity for identifying BPO and the other BOD subtype. In patients with LUTS and small to moderate prostate volume, invasive video urodynamic study is still necessary when invasive treatment modality is recommended.
Table 1. Diagnostic performance of the prediction models for the BOD subtypes in the training, internal validation, and test sets
|
|
Stage I model |
Stage II model |
|||
|
|
BOD |
BND |
BPO |
DV |
PRES |
|
Training set |
|
|
|
|
|
|
AUC |
0.71 |
0.70 |
0.85 |
0.84 |
0.83 |
|
Threshold of training set |
0.78 |
0.40 |
0.35 |
0.17 |
0.23 |
|
Accuracy |
0.73 |
0.68 |
0.82 |
0.72 |
0.81 |
|
Sensitivity |
0.77 |
0.88 |
0.75 |
0.95 |
0.81 |
|
Specificity |
0.55 |
0.49 |
0.86 |
0.66 |
0.81 |
|
PPV |
0.89 |
0.61 |
0.74 |
0.41 |
0.52 |
|
NPV |
0.34 |
0.82 |
0.87 |
0.98 |
0.94 |
|
AUC |
0.70±0.10 |
0.70±0.07 |
0.84±0.07 |
0.80±0.06 |
0.81±0.08 |
|
Accuracy |
0.74±0.06 |
0.66±0.06 |
0.81±0.06 |
0.68±0.07 |
0.78±0.06 |
|
Test set |
|
|
|
|
|
|
AUC |
0.70 |
0.68 |
0.79 |
0.61 |
0.73 |
|
Accuracy |
0.74 |
0.60 |
0.73 |
0.63 |
0.80 |
|
Sensitivity |
0.80 |
0.83 |
0.58 |
0.71 |
0.33 |
|
Specificity |
0.47 |
0.38 |
0.82 |
0.62 |
0.84 |
|
PPV |
0.87 |
0.56 |
0.63 |
0.16 |
0.15 |
|
NPV |
0.35 |
0.71 |
0.78 |
0.95 |
0.94 |
DV and PRES models were developed using SMOTE to address class imbalance (DV: non-DV = 40:160; PRES: non-PRES = 41:162).
The reported AUCs are based on the resampled datasets.
AUC: Area under the receiver operating characteristic curve, BOD: bladder outlet dysfunction; BND: bladder neck dysfunction, BPO: benign prostatic obstruction, DV: dysfunctional voiding, NPV: negative predictive value, PPV: positive predictive value, PRES: poor relaxation of external sphincter, SMOTE: synthetic minority over-sampling technique
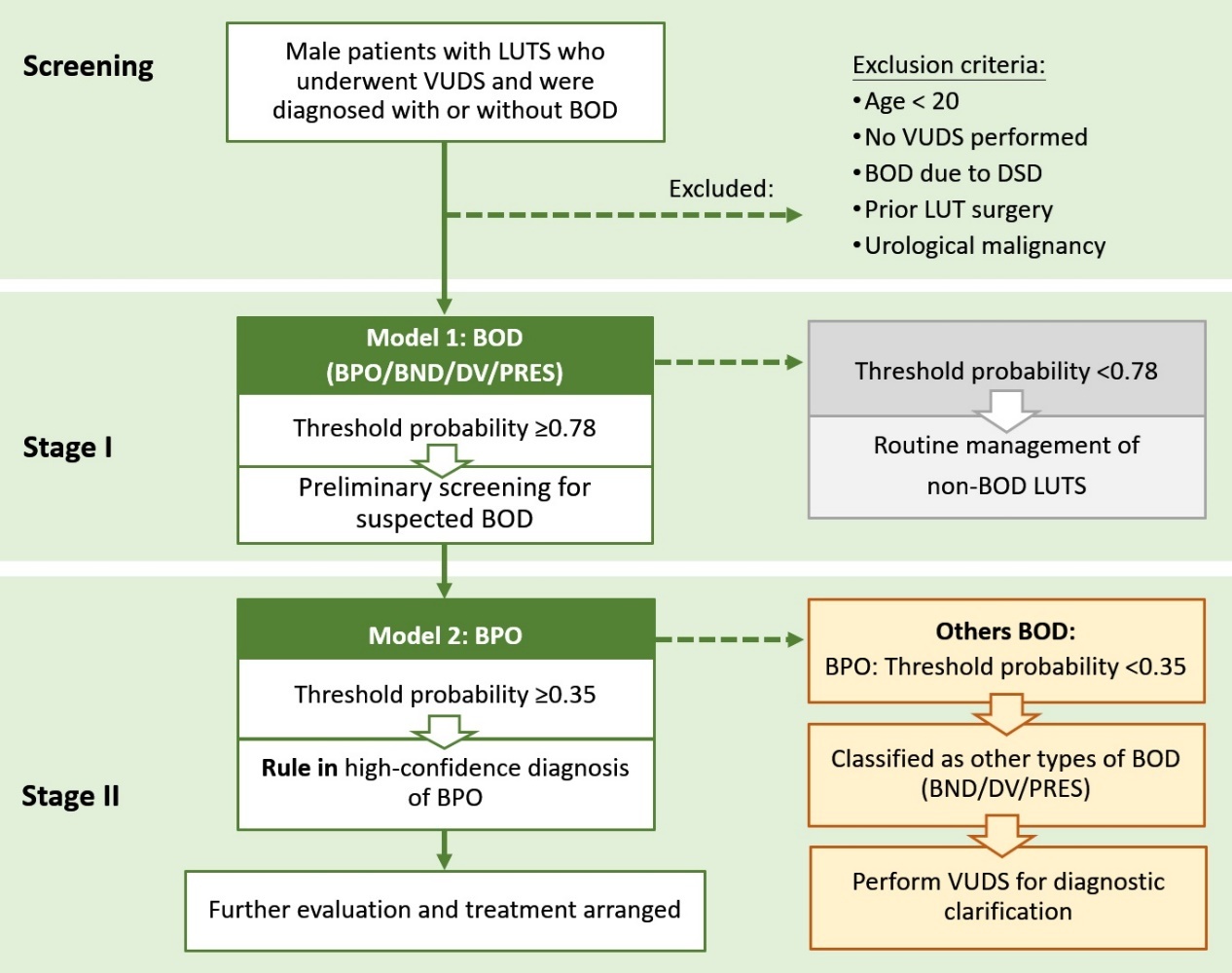
Figure 1. A two-stage model decision-making framework. Bladder outlet dysfunction (BOD) includes the following: benign prostate obstruction (BPO), bladder neck dysfunction (BND), dysfunctional voiding (DV), and poor external sphincter relaxation (PRES). VUDS: video urodynamic study