泌尿道尿路上皮癌接受下腔靜脈切除與左腎靜脈重建後成功保留腎功能:病例報告
1,3曾義翔、1,3魏子鈞、1,3張延驊、2賴峻毅、1,3黃逸修
¹ 臺北榮民總醫院泌尿部
² 臺北榮民總醫院腫瘤醫學部
³國立陽明交通大學醫學院泌尿學科及書田泌尿科學研究中心
Successful preservation of renal function after suprarenal-to-bifurcation IVC resection and left renal vein reconstruction in high-grade upper tract urothelial carcinoma
1I-Hsiang Tseng, 1,3Tzu-Chun Wei, 1,3Yen-Hwa Chang, 2Jiun-I Lai,
1,3Eric Yi-Hsiu Huang,
1Department of Urology, 2Department of oncology,
Taipei Veterans General Hospital, Taipei, Taiwan
3Department of Urology, College of Medicine and ShuTien Urological Research Center, National Yang Ming Chiao Tung University, Taipei, Taiwan
Abstract
Introduction
Upper tract urothelial carcinoma (UTUC) accounts for approximately 5–10% of all urothelial malignancies and typically spreads through local extension or lymphatic dissemination rather than venous pathways. Direct renal vein or inferior vena cava (IVC) involvement is exceedingly rare—far less common than in renal cell carcinoma—with only isolated case reports documenting UTUC extending into the renal vein or caval system. Due to this rarity, optimal strategies for vascular resection, reconstruction, and perioperative renal protection remain poorly defined.
For patients with advanced or unresectable UTUC, systemic therapy remains the standard of care, including platinum-based chemotherapy, immune checkpoint inhibitors, and antibody–drug conjugates. In selected cases, disease stabilization achieved through systemic treatment may allow consideration of consolidative or conversion surgery. However, performing radical nephroureterectomy in the presence of extensive IVC involvement introduces substantial technical challenges, including the need for segmental caval resection, renal venous reconstruction, temporary extracorporeal support, and preservation of renal function.
We report a rare case of high-grade UTUC with radiologically and intraoperatively confirmed IVC involvement, including extension into the right renal vein and a long suprarenal caval segment. The patient underwent radical nephroureterectomy, extensive IVC resection from the suprarenal level to the bifurcation and left renal vein reconstruction using a handmade bovine-patch conduit under veno-venous ECMO support. This case highlights the feasibility of aggressive vascular surgery and demonstrates successful preservation of renal function despite extensive interruption of the caval system.
Case presentation
A 60-year-old woman presented with intermittent painless gross hematuria beginning in March 2024. CT imaging revealed a 4 cm heterogeneously enhancing mass in the right renal pelvis with extension and encasement of the right renal vein and inferior vena cava (IVC), upstream hydronephrosis, and borderline retroperitoneal lymphadenopathy (Figure 1). No distant metastasis was detected. A CT-guided biopsy confirmed high-grade urothelial carcinoma.
She subsequently underwent multiple lines of systemic therapy, including pembrolizumab, pembrolizumab plus enfortumab vedotin, gemcitabine/cisplatin (dose-adjusted for renal impairment), and later avelumab maintenance. Despite therapy, serial imaging showed persistent locally advanced disease with continued IVC involvement, including the right renal vein and suprarenal IVC, accompanied by suspected partial IVC thrombosis.
In September 2025, she underwent open radical nephroureterectomy with en bloc resection of the involved IVC segment. Intraoperatively, the tumor extensively infiltrated the right renal pelvis, renal sinus, right renal vein, and IVC. Dense adhesions to the duodenum were noted. The IVC was transected from the suprarenal level down to the bifurcation, and the infrarenal IVC was ligated due to chronic obstruction. Temporary veno-venous ECMO was used during vascular control. The left renal vein was reconstructed to the suprarenal IVC using a hand-sewn bovine patch conduit (Figure 2&3).
Postoperatively, renal function demonstrated a transient mild rise in serum creatinine from a preoperative value of 1.98 mg/dL to a peak of 2.49 mg/dL on postoperative day (POD) 1-2, followed by steady improvement to 2.04 mg/dL on POD 3 and 1.91 mg/dL on POD 4. No dialysis was required. She recovered uneventfully and was discharged in stable condition.
Pathology confirmed high-grade invasive urothelial carcinoma of the renal pelvis with renal sinus involvement (pT3) and metastatic carcinoma in 2 of 9 hilar lymph nodes (pN2). All surgical margins were negative.
Discussion
IVC involvement by UTUC is exceptionally rare, with the literature limited to sporadic case reports describing renal pelvic tumors extending into the renal vein or caval lumen ADDIN EN.CITE <EndNote><Cite><Author>Tseng</Author><Year>2010</Year><RecNum>32</RecNum><DisplayText>[4]</DisplayText><record><rec-number>32</rec-number><foreign-keys><key app="EN" db-id="9dwxxxxsz55rdzes2t5vravjz9dzr5r99xr0" timestamp="1763891786">32</key></foreign-keys><ref-type name="Journal Article">17</ref-type><contributors><authors><author>Tseng, Y. S.</author><author>Chen, K. H.</author><author>Chiu, B.</author><author>Chen, Y.</author><author>Chung, S. D.</author></authors></contributors><auth-address>Department of Surgery, Far Eastern Memorial Hospital, Banciao, Taipei, Taiwan.</auth-address><titles><title>Renal urothelial carcinoma with extended venous thrombus</title><secondary-title>South Med J</secondary-title></titles><periodical><full-title>South Med J</full-title></periodical><pages>813-4</pages><volume>103</volume><number>8</number><keywords><keyword>Hematuria/etiology</keyword><keyword>Humans</keyword><keyword>Male</keyword><keyword>Middle Aged</keyword><keyword>Renal Veins/pathology</keyword><keyword>Urologic Neoplasms/*complications/diagnosis/pathology</keyword><keyword>Urothelium/*pathology</keyword><keyword>Vena Cava, Inferior/pathology</keyword><keyword>Venous Thrombosis/*etiology/pathology</keyword></keywords><dates><year>2010</year><pub-dates><date>Aug</date></pub-dates></dates><isbn>1541-8243 (Electronic)
0038-4348 (Linking)</isbn><accession-num>20622737</accession-num><urls><related-urls><url>https://www.ncbi.nlm.nih.gov/pubmed/20622737</url></related-urls></urls><electronic-resource-num>10.1097/SMJ.0b013e3181e63393</electronic-resource-num><remote-database-name>Medline</remote-database-name><remote-database-provider>NLM</remote-database-provider></record></Cite></EndNote>[4] ADDIN EN.CITE ADDIN EN.CITE.DATA [5]. This pattern contrasts sharply with renal cell carcinoma, where venous extension is relatively frequent and surgical strategies are well-established.
The extensive tumor burden in this patient necessitated segmental IVC resection from the suprarenal region to the bifurcation, an approach primarily described in complex urologic–vascular surgery ADDIN EN.CITE ADDIN EN.CITE.DATA [7] ADDIN EN.CITE ADDIN EN.CITE.DATA [8] . Chronic infrarenal IVC obstruction, recognized intraoperatively, likely promoted collateral venous development, facilitating hemodynamic tolerance during caval interruption. Temporary veno-venous ECMO support—an adjunct occasionally employed in major venous reconstructions when conventional bypass is insufficient—provided stable venous return during prolonged clamping ADDIN EN.CITE ADDIN EN.CITE.DATA [8] ADDIN EN.CITE ADDIN EN.CITE.DATA [9].
Preservation of renal function during caval surgery depends critically on maintaining adequate renal venous drainage. Although left renal vein (LRV) ligation can be tolerated when robust lumbar, adrenal, and gonadal venous collaterals are present, the risk of renal congestion and postoperative dysfunction remains significant. Recent studies demonstrate stable renal function after LRV ligation only when extensive collateral pathways are confirmed ADDIN EN.CITE ADDIN EN.CITE.DATA [10]. In this case, LRV reconstruction using a bovine-patch conduit, combined with pre-existing collaterals, enabled preservation of renal outflow and rapid normalization of postoperative creatinine.
The patient underwent multiple systemic therapies, including immune checkpoint inhibition, platinum-based chemotherapy, and antibody–drug conjugate therapy. Contemporary multimodal regimens may improve local and nodal disease control and allow some patients to undergo consolidative surgery ADDIN EN.CITE ADDIN EN.CITE.DATA [5] ADDIN EN.CITE ADDIN EN.CITE.DATA [6]. Although evidence remains limited for UTUC with IVC involvement, this case underscores the potential role of multimodal therapy followed by aggressive urologic–vascular surgery in selected patients.
Conclusion
This case illustrates that radical nephroureterectomy combined with extensive IVC resection and individualized renal venous reconstruction can be safely performed in carefully selected patients with UTUC exhibiting IVC involvement. Successful preservation of postoperative renal function underscores the importance of meticulous preoperative vascular assessment, evaluation of collateral venous pathways, and the judicious use of extracorporeal support. These findings highlight the potential role of aggressive, well-planned urologic–vascular surgical strategies as part of multimodal management for complex UTUC presentations involving the caval system.
Figure
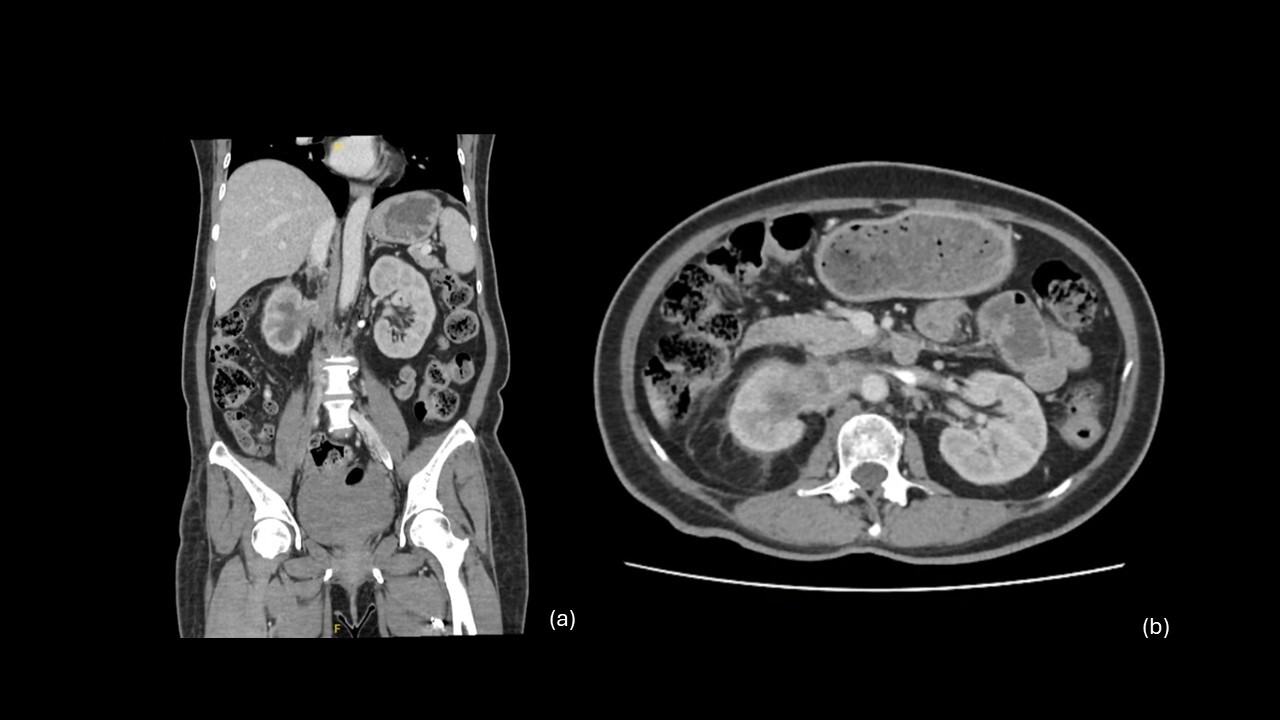
Figure 1.
(a) Coronal CT demonstrates a right renal pelvic mass with extension into the right renal vein and suprarenal inferior vena cava (IVC).
(b) Axial CT showing the tumor encasing the right renal vein with associated IVC involvement.
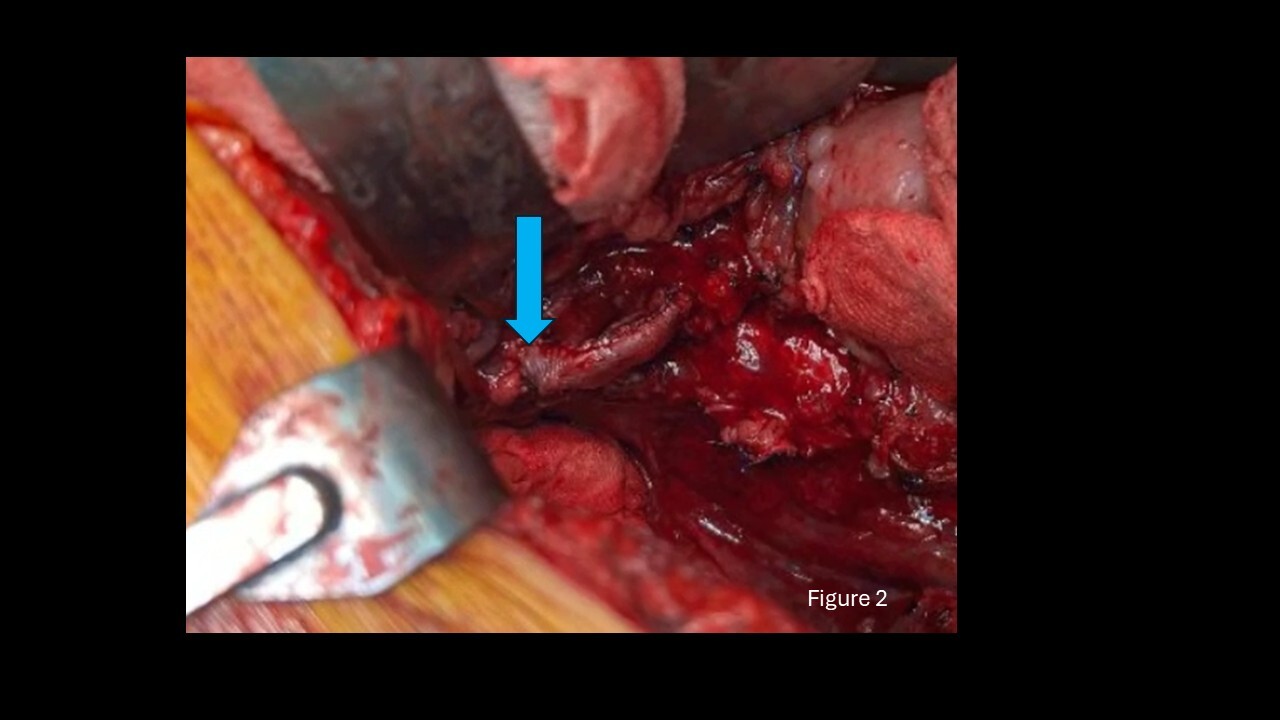
Figure 2. Intraoperative view showing the hand-sewn bovine patch conduit (blue arrow)
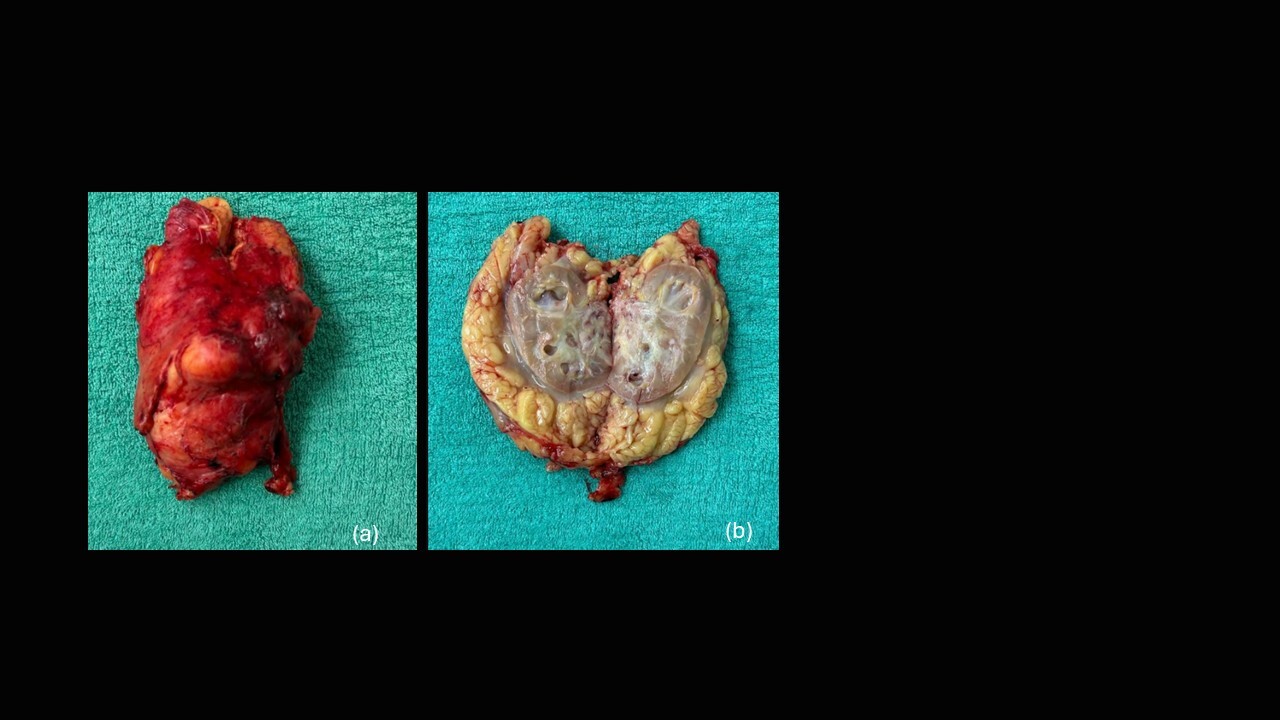
Figure 3. Gross specimen of the right kidney and perinephric tissue.
(a) Intact specimen following radical nephroureterectomy.
(b) Bisected kidney showing the tumor occupying the renal pelvis and invading the renal parenchyma.